
CT Diagnosis and Differentiation Between Primary Hepatic Vein Budd-Chiari Syndrome and Hepatic Sinusoidal Obstructive Syndrome
-
摘要:
目的:原发性肝静脉型布加综合征与肝窦阻塞综合征的临床表现及实验室检查缺乏特异性,影像学表现相似,本研究通过收集BCS及SOS的临床及影像特点,探讨增强CT在两种疾病的鉴别诊断的应用。材料与方法:回顾分析经DSA确诊的26例BCS和经肝活检确诊的20例SOS患者的临床及影像资料,比较其差异。结果:BCS患者门脉高压相关表现较明显,肝动脉直径、门脉主干直径及脾静脉增宽程度均超过SOS患者;CT增强扫描16例BCS患者呈现出门脉期以第一肝门及尾状叶为主出现斑片状强化方式;11例SOS患者门脉期则呈现出以第二肝门为中心的“鸦爪样”不均质强化方式;BCS肝功能损伤相对较轻于SOS患者,SOS患者的碱性磷酸酶增高、总胆固醇增高、白蛋白减低程度较BCS患者相对明显。两者病例影像的共同点是静脉期三支肝静脉不显影或显影纤细。结论:CT平扫及增强检查对BCS和SOS有重要意义,尾状叶体积改变、侧支循环开放程度等都是二者CT鉴别诊断要点,特别是增强CT所示的BCS呈现以第一肝门为中心不均匀强化方式及SOS以第二肝门为中心的不均匀强化方式有助于疾病早期的鉴别诊断。
-
关键词:
- 原发性肝静脉型布加综合征 /
- 肝窦阻塞综合征 /
- 体层摄影术 /
- X线计算机 /
- 鉴别诊断
Abstract:Objective: The clinical and laboratory specificity for diagnosing Budd-Chiari syndrome (BCS) and hepatic sinusoidal obstructive syndrome (SOS) is limited. This study aims to explore the application of contrast-enhanced CT in the differential diagnosis of BCS and SOS by examining their clinical and imaging features. Materials and Methods: Clinical and imaging data from 26 patients diagnosed with BCS via DSA and 20 patients diagnosed with SOS via liver biopsy were retrospectively analyzed. The differences between the two groups were compared. Results: Portal hypertension-related symptoms were more prominent in 16 patients with BCS, and the diameter of the hepatic artery, portal trunk, and degree of splenic vein dilation were all greater than those in 11 patients with SOS. On contrast-enhanced CT, BCS exhibited a patchy enhancement pattern in the portal phase, primarily localized to the first hepatic portal and caudate lobe. In contrast, SOS showed a "crow's claw-like" heterogeneous enhancement pattern centered on the second hepatic division. Liver function injury in BCS patients was less severe than in SOS patients. Elevated alkaline phosphatase, increased total cholesterol, and decreased albumin levels were more pronounced in SOS patients compared to those with BCS. A common feature in both groups was the absence or faint visibility of the three hepatic veins in the venous phase. Conclusion: The CT findings of BCS and hepatic SOS exhibit certain specificities. The enlargement of the caudate lobe and the degree of collateral circulation are key factors in the CT-based differential diagnosis. Notably, the heterogeneous enhancement pattern of BCS centered on the first hepatic portal and the heterogeneous enhancement pattern of SOS centered on the second hepatic portal in contrast-enhanced CT are valuable for the early differential diagnosis of these conditions.
-
双能量CT(dual-energy computed tomography, DECT)作为一种较为先进的成像技术,已广泛应用于临床实践。DECT利用物质在不同X射线能量下的衰减特性,获取高能量和低能量图像数据,从而实现单能量成像、物质成分分离和定量分析[1-3]。
在物质的定量分析中,电子密度(electron density, ED)ρe和有效原子序数(effective atomic number, EAN)Zeff不仅用于结石成分分类和肿瘤良恶性鉴别,还被用于放射治疗的蒙特卡洛剂量估算和放疗后放射性肺炎的分级评估[4-9]。因此,准确测量ρe和Zeff是实现精准影像诊断和精确剂量估算的基础。虽然已有一些研究探讨了在DECT中测量ρe和Zeff的准确性,但由于使用的CT机型(双能量成像模式)、扫描和重建参数等存在差异,导致这些研究结果难以进行比较。
本文综述近年来相关的文献研究,分析影响ρe和Zeff测量准确性的关键因素,探讨提高这些参数测量精度的方法,旨在提高影像诊断和治疗的精确性。
1. ρe和Zeff的影响因素
常规CT图像的生成是基于不同物质对X射线的衰减程度的差异,这些差异通常用衰减系数μ来量化,并以Hounsfield单位(HU)表示。因此在临床实践中,组织的HU值可能会因光子能量和扫描参数的变化而发生改变。此外,不同的组织也会表现出相同的HU值,这种现象源于衰减系数μ不仅受到光子能量的影响,还与组织密度和元素组成密切相关。1976年,Rutherford 等[10]提出利用不同能量的X射线对同一解剖结构进行至少两次扫描,以获取不同能量下的图像,进而推导出衰减系数μ与ρe和Zeff之间的关系。
目前,双能量成像作为主流的能谱CT技术,其X射线能量的解析方法会间接影响ρe和Zeff的计算结果。能量解析主要有两种方法:基于投影数据域的解析和基于图像域的解析[11]。前者通过减少射线束硬化效应,提高了解析的准确性,但计算过程更为复杂且对噪声更加敏感;后者则在计算简便性和对噪声的抗干扰能力上具有优势[12]。总之,射线束硬化效应和噪声都可能对物质的衰减系数μ造成干扰,进而影响对组织ρe和Zeff的测量精度。
1.1 射线束硬化效应的影响
CT系统采用多色能谱X射线技术,在X射线穿透介质的过程中,大量低能X射线被吸收衰减,而高能X射线的衰减相对较少,导致透射线束中的高能X射线比例提高,出现“射线束硬化”的现象[13]。在这过程中,衰减系数μ发生了变化。然而,在图像重建过程中,通常假设X射线能谱为单色,即认为衰减系数μ是恒定不变的。这种假设会导致实际的衰减系数μ与假定值之间出现偏差,进而影响到ρe和Zeff的测量精度。
随着被测物体体积的增大,射线束硬化效应变得更加显著,这将导致ρe和Zeff的测量误差进一步增大。Schaeffer等[14]在研究中指出,在较小尺寸的头部模型中,ρe和Zeff的测量值比在较大尺寸的体部模型中更为精确。然而,Almeida等[15]的研究结果与之不同,在两种不同尺寸的模型中,ρe和Zeff的测量值并无显著差异,这可能源于事先使用模体进行了ρe和Zeff的校准,有效地校正了射线束硬化效应。值得注意的是,尽管Hua等[16]没有使用模体进行校准,但他们的研究结果与Almeida等[15]相似,发现两种尺寸模型中ρe和Zeff的测量值差异控制在0.7% 和2% 以内。这可能与他们使用的双层探测器CT技术有关,该技术能够实现基于投影数据的材料分解,有效减轻射线束硬化的影响。
除体型尺寸外,扫描中心的偏移也是影响射线束硬化效应的一个重要因素。Schaeffer等[14]发现,当模体在上下左右4个方向上发生偏移时,Zeff会有 3% 的变化,而ρe则相对不敏感。尽管Zeff的变化幅度不大,但这足以对物质的鉴别造成影响。例如,在偏离等中心点的模体中,血液等效组织插件(40 HU)的Zeff与未发生偏移模体中的水等效组织插件的Zeff相近。由于扫描位置受到受检者特异性及摆位技师判断偏倚的影响,难以通过其他方法进行校正,因此,制定标准化的摆位流程对于提高ρe和Zeff测量的准确性至关重要。
1.2 噪声的影响
噪声具有随机性、不确定性,会干扰正常信号的接收与处理。在CT成像领域,噪声的存在不仅影响图像的纹理,还会导致衰减系数μ的测量值与其真实值之间存在偏差。在临床实践中,降低噪声对于提升CT图像质量至关重要。为了减少噪声对衰减系数μ测量的影响,提高ρe和Zeff的测量精度,选择恰当的扫描参数和应用高效的噪声抑制技术显得尤为关键。
CT噪声主要与探测器接收的X射线光子量有关,增加X射线能量或扫描剂量可以降低噪声水平。Landry等[17]的研究表明,随着曝光剂量的增加,模体中脂肪、水、肌肉等效组织插件的ρe和Zeff的区分度提高,同时在近距离放疗的蒙特卡洛模拟中,剂量计算的误差也相应减小。然而,Hua等[16]的研究发现,在不同的管电压和剂量水平下,ρe和Zeff的测量展现出较高的准确性和稳定性。这一结果可能与Hua等[16]使用的曝光剂量范围较窄,而Landry等[17]则采用了0.5至4倍的剂量范围有关。
除了剂量和能量外,迭代算法也是影响CT噪声的关键因素。与传统的滤波反投影(filtered back projection,FBP)算法相比,迭代重建算法有效地降低了图像噪声并提高了图像质量[18-20]。Landry等[17]发现正弦图确定迭代重建(sinogram-affirmed iterative reconstruction,SAFIRE)算法在降低ρe和Zeff的标准偏差方面表现优于FBP算法,尤其在使用最大强度时。也有其他研究指出,ρe和Zeff的测量精度与迭代重建算法的强度并无明显关联[16,21],这可能与不同研究中使用的CT机品牌和型号有关。
除了上述参数,层厚、螺距、旋转时间、卷积核等其他扫描参数同样对CT噪声有着显著影响,这些因素对ρe和Zeff测量准确性的影响值得进一步研究和探讨。
2. 不同双能量成像模式CT对ρe和Zeff的测量研究
根据不同的双能量实现方式,DECT可分为单源瞬时管电压切换模式、单源序列扫描模式、双源双能量扫描模式、单源双光束模式和单源双层探测器模式[22](图1)。DECT通过获取物质在两种不同能量下的X射线衰减信息,利用物质在不同能量下的衰减差异进行物质分解和定量分析(图2和图3)。
![]()
![]() 图 3 电子密度和有效原子序数在胆脂瘤患者中的应用注:女,61岁,胆脂瘤伴肉芽肿。Figure 3. Application of electron density and effective atomic number in patients with cholesteatoma.
图 3 电子密度和有效原子序数在胆脂瘤患者中的应用注:女,61岁,胆脂瘤伴肉芽肿。Figure 3. Application of electron density and effective atomic number in patients with cholesteatoma.(1)单源瞬时管电压切换模式DECT可在机架旋转期间实现高低电压的快速切换,尽管X射线投影角度几乎相同,允许基于投影数据域进行能量解析,但由于时间分辨力的损失,会在一定程度上影响能量解析的准确性。
当前的研究在评估Zeff测量的准确性方面展现了不同结果[21,24,25]。例如,Goodsitt等[24]通过模体实验得出Zeff的测量相对误差控制在15% 以内的结论。相对地,Kawahara等[25]报告称Zeff的测量相对误差在5.1% 以内。这种差异可能是因为各研究中所采用的CT机型和扫描参数不同,以及模体材料和结构的多样性所致。在ρe测量的准确性方面,Ogata等[26]发现在不同单能级图像中,模体所有材料的ρe测量相对误差控制在1.1% 以内。目前,基于单源瞬时管电压切换模式的DECT测量ρe准确性的研究相对较少,未来可进一步探索。
(2)单源序列扫描模式DECT分别以高、低能量进行两次扫描实现双能量成像。两套独立的高低能量图像具有完全的能量分离效果,这种特性有助于提高ρe和Zeff的测量准确性。当前,相关研究表明ρe和Zeff的测定具有较高的精度,有助于提高放射治疗计划的准确性[14,27-29]。其中Schaeffer等[14]基于模体实验发现Zeff的测量相对误差为3.2%,并且认为与Kawahara等[25]基于单源瞬时管电压切换模式 DECT的研究结果相似(Zeff的测量相对误差为2.5%)。
在单源序列扫描成像模式下,两次球管旋转扫描之间存在一定的时间(如某品牌CT高低管电压扫描间隔为180~800 ms[28]),可能会影响空间配准效果,并且在临床实践中由于受到受检者运动的影响,导致材料分解存在偏差[30]。此外,较大的能谱分离效果有助于产生更好的材料区分效果,提高ρe和Zeff的准确性。目前单源序列扫描模式DECT的高能量成像多采用135 kVp的管电压,能谱分离效果略低于单源瞬时管电压切换模式DECT的140 kVp[25]。
(3)双源双能量扫描模式DECT具有较大的能谱分离优势,它采用两套X射线球管和探测器,对同一解剖平面分别发射高、低管电压的X射线并由相应的探测器采集数据。
随着技术的进步,目前双源DECT多采用能谱纯化技术进一步增大能谱分离效果,减少射线束硬化伪影,提高了ρe和Zeff的测量准确性[15,31-32]。然而,两套探测器的空间位置设计也会对ρe和Zeff的测量带来一定的影响,仅35.5 cm的全扫描视野,对于超力型成年受检者的ρe和Zeff的测量具有局限性。此外,鉴于高、低能量数据采集的相位差异,该双能量CT采用了一种对噪声反应更为敏感的图像域能量解析技术。然而,当两套探测器同时捕获高能和低能X射线时,交叉散射的产生是不可避免的,这种散射会加剧噪声,从而可能对ρe和Zeff的精确测量带来不利影响。
(4)单源双光束模式DECT采用分离滤波技术,使X射线束预先分离成高、低能量的两种光子束,由对应位置的探测器沿Z轴方向分别接收,使得同一解剖区域接收高、低能两种X射线束存在时间差异,同样地基于图像域进行能量解析。尽管该模式DECT在成像过程中也容易受到光子交叉、散射等影响,但是相关研究发现单源双光束模式DECT在测量ρe和Zeff的准确性方面劣于双源DECT[15]。该研究发现第2代、第3代双源DECT的ρe和Zeff的测量相对误差分别在1.2% 和6.2% 以内,然而单源双光束DECT的ρe和Zeff的测量相对误差最大可达15.3% 和28.1%。较大的测量误差可能源于单源双光束DECT的高能和低能数据均源自相同的管电压设置,这种设计导致能谱分离效果相对较弱,从而使得成像系统对图像噪声和伪影更为敏感,影响了ρe和Zeff的准确性。
(5)单源双层探测器模式DECT同样对高能和低能数据采用了相同的管电压设置,并且存在使用相同管电流所致的高、低能光谱图像的噪声水平不同的局限,但相关研究显示出了稳健的ρe和Zeff的测量准确性[16,33]。
Hua等[16]基于模体实验发现ρe的测量相对误差范围在 -0.1% 至1.1%,Zeff的测量相对误差范围为 -2.3% 至1.7%。这些发现可以归因于该模式的DECT采用了独特的设计:一个X射线球管与空间上对称分布的上下两层探测器相结合。这种双层探测器配置能够同步捕获高、低能量的X射线信息,实现了基于投影数据域的材料分解[34]。从理论上讲,这种方法相较于基于图像域的材料分解具有一定的优势。
3. 总结与展望
DECT根据不同能量下物质衰减系数μ的差异进行物质分解,以实现单能量CT扫描无法评估的物质特性,其中ρe和Zeff在评估材料特性和放疗剂量估算中发挥着重要的作用。本文重点探讨影响ρe和Zeff测量精度的射线束硬化效应和噪声两大关键因素,并详细分析不同双能量成像模式CT对ρe和Zeff测量准确性的具体影响,明确了各成像模式的优势与局限。
鉴于此,未来的研究需进一步探索和优化算法,以减轻射线束硬化效应和噪声的不利影响,从而提升图像质量和测量的精确度。同时,由于不同双能量成像模式CT对ρe和Zeff测量准确性的差异化影响,未来的工作还需对这些成像模式进行细致的比较研究,并针对不同双能量成像模式CT,探索所使用机型的最佳成像条件以提高ρe和Zeff的测量准确性。
-
![]()
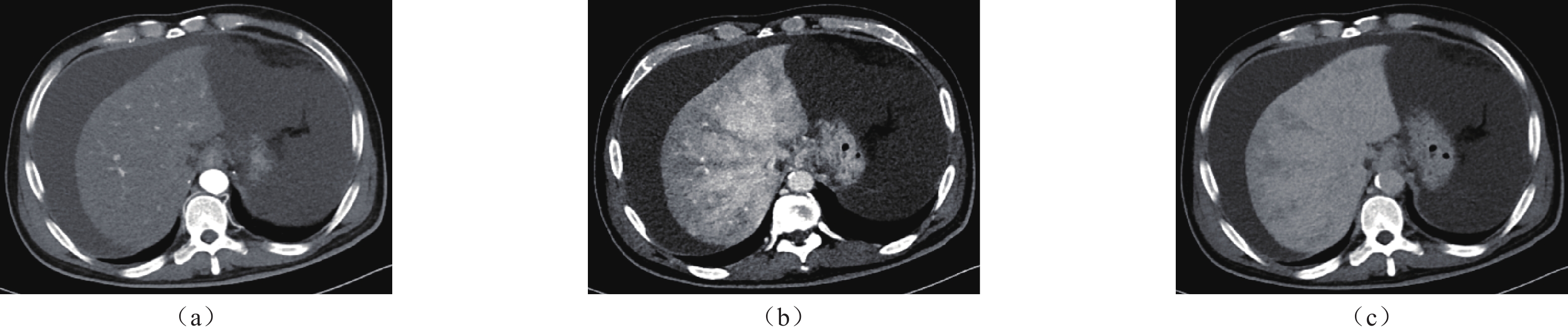
图 1 BCS CT增强检查特征性表现,男19岁,经DSA检查确诊为BCS,CT增强扫描动脉期(a)肝实质轻度均匀强化,门脉期(b)肝实质以第一肝门和尾状叶为主明显强化,延迟期(c)延迟期强化范围较前增大。
Figure 1. Characteristic findings of Budd-Chiari syndrome (BCS) on Contrast-Enhanced CT. A 19-year-old male, diagnosed with BCS via DS, underwent enhanced CT. The arterial phase (1A) showed mild homogeneous enhancement in the hepatic parenchyma, while the portal phase (1B) revealed significant enhancement in the first hepatic portal and caudate lobe. In the delayed phase (1C), the enhancement range was notably increased.
![]()
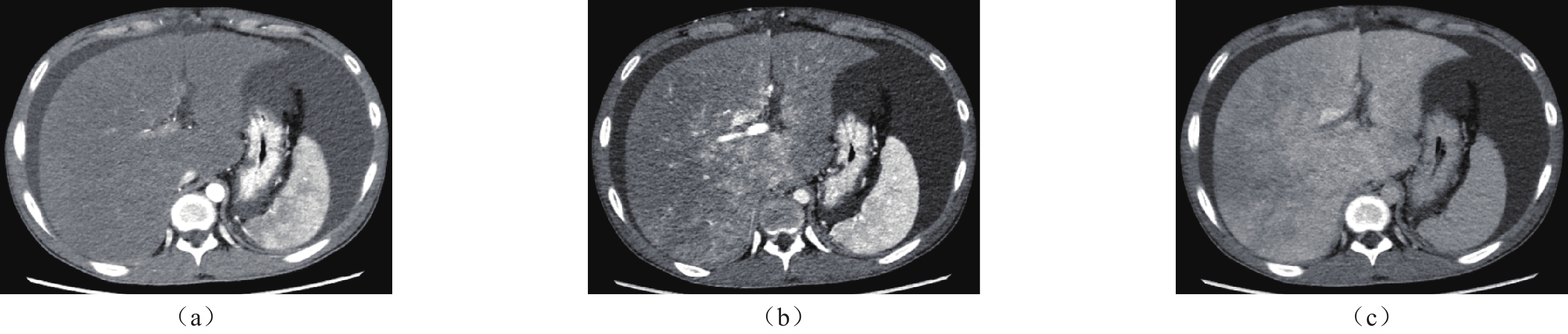
图 2 SOS CT增强检查特征性表现. 男49岁,经肝穿确诊为SOS,CT增强扫描动脉期(a)肝实质轻度均匀强化,门脉期(b)肝实质以第二肝门为中心的“鸦爪样”不均质强化,延迟期(c)延迟期强化范围较前增大。
Figure 2. Characteristic findings of hepatic sinusoidal destructive syndrome (SOS) on contrast-enhanced CT. A 49-year-old male, diagnosed with SOS via liver biopsy, underwent contrast-enhanced CT. The arterial phase (2A) showed mild homogeneous enhancement in the liver parenchyma, while the portal phase (2B) revealed a “raven’s paw” heterogeneous enhancement pattern centered on the second hepatic hilum.
表 1 两组患者的实验室检查(%)
Table 1 Laboratory tests between the two groups (%)
天冬氨酸
转氨酶 > 35 U/L丙氨酸
转氨酶 > 40 U/L碱性磷
酸酶 > 135 U/Lγ-谷氨酰
转肽酶 > 45 U/L总胆红素 > 17.1 umol/l 总胆固醇>5.7 mm/L 白蛋白 < 35 g/l 凝血酶
原时间 > 13 S)血小板 < 100×
109CA125
(升高)>
正常值
2 倍尿蛋白
(+)原发性
肝静脉
型布加
综合征44 8 31 73 85 0 50 77 36 45 0 肝静脉
闭塞
综合征45 30 60 90 90 15 85 70 35 65 5  下载: 导出CSV
下载: 导出CSV
表 2 两种疾病的影像学特征
Table 2 Imaging features of the two groups
类别 原发性肝静脉型布加综合征 肝窦阻塞综合征 CT平扫 肝脏肿大,肝实质密度不均匀减低,多伴腹水形成 肝脏肿大,肝实质密度不均匀减低,多伴腹水形成 CT增强
动脉期肝实质均未见明显强化或呈轻度强化方式 肝实质均未见明显强化或呈轻度强化方式 门脉期 以第一肝门及尾状叶为主出现斑片状强化 第二肝门为中心的“鸦爪样”不均质强化 延迟期 肝实质仍呈斑片状强化,强化范围较门脉期进一步增大 肝实质仍呈“鸦爪样”强化,强化范围较门脉期进一步增大 肝静脉显影 未见显影、部分显影或纤细 未见显影、部分显影或纤细 肝动脉直径/mm 4.695±0.70 4.00±0.83 门静脉直径/mm 12.42±2.17 9.73±1.93
下载: 导出CSV
-
[1] FERRAL H, BEHRENS G, LOPERA J. Budd-chiari syndrome[J]. American Journal of Roentgenology, 2012, 199(4): 737-745. DOI: 10.2214/AJR.12.9098.
[2] LUPESCU I G, DOBROMIR C, POPA G A, et al. Spiral computed tomography and magnetic resonance angiography evaluation in Budd-Chiari syndrome[J]. Journal of Gastrointestinal and Liver Diseases, 2008, 17(2): 223-226. DOI: DOI: 10.1111/j.1440-1746.2008.05468.x.
[3] CAZALS-HATEM D, VALÉRIE VILGRAIN, GENIN P, et al. Arterial and portal circulation and parenchymal changes in Budd-Chiari syndrome: A study in 17 explanted livers[J]. Hepatology, 2003, 37(3). DOI: 10.1053/jhep.2003.50076.
[4] OFLIVER E A F. EASL clinical practice guidelines: Vascular diseases of the liver[J]. Journal of Hepatology, 2016, 64(1): 179-202. DOI: 10.1016/j.jhep.2015.07.040.
[5] XUE H, LI Y C, SHAKYA P, et al. The role of intravascular intervention in the management of budd-chiari syndrome[J]. Digestive Diseases and Sciences, 2010, 55(9): 2659-2663. DOI: 10.1007/s10620-009-1087-7.
[6] CORBACIOGLU S, JABBOUR E J, MOHTY M. Risk factors for development of and progression of hepatic veno-occlusive disease/sinusoidal obstruction syndrome[J]. Biology of Blood and Marrow Transplantation, 2019, 25(7): 1271-80. DOI: 10.1016/j.bbmt.2019.02.018.
[7] VALLA D C, CAZALS-HATEM D. Sinusoidal obstruction syndrome[J]. Clinics and Research in Hepatology and Gastroenterology, 2016: 378-385 . DOI: 10.1016/j.clinre.2016.01.006.
[8] 范春蕾, 丁惠国, 王文娟, 等. 非造血干细胞移植肝窦阻塞综合征患者的临床特征分析[J]. 北京医学, 2018, 40(10): 5. DOI:CNKI: SUN:BJYX.0.2018-10-005. FAN C L, DING H G, WANG W J. Clinical features of patients with sinusoidal obstruction syndrome without hematopoietic stem cell transplantation[J]. Beijing Medical Journal, 2018, 40(10): 5. DOI:CNKI:SUN:BJYX.0.2018-10-005. (in Chinese).
[9] SHIN J, YOON H, CHA Y J, et al. Liver stiffness and perfusion changes for hepatic sinusoidal obstruction syndrome in rabbit model[J]. World Journal of Gastroenterology, 2020, 26(7): 706-16. DOI: 10.3748/wjg.v26.i7.706.
[10] NORTHUP P G, GARCIA-PAGAN J C, GARCIA-TSAO G, et al. Vascular liver disorders, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the american association for the study of liver diseases[J]. Hepatology (Baltimore, Md), 2021, 73(1): 366-413. DOI: 10.1002/hep.31646.
[11] LIN G, WANG J Y, LI N, et al. Hepatic sinusoidal obstruction syndrome associated with consumption of Gynura segetum[J]. Journal of Hepatology, 2011, 54(4): 666-673. DOI: 10.1016/j.jhep.2010.07.031.
[12] VALLA D C. Budd-Chiari syndrome/hepatic venous outflow tract obstruction[J]. Hepatology International, 2017, 12(S1). DOI: 10.1007/978-3-319-23018-4_39.
[13] FAN J, WANG Q, LUO B, et al. Prevalence of prothrombotic factors in patients with budd-chiari syndrome or non-cirrhotic nonmalignant portal vein thrombosis: A hospital-based observational study[J]. Journal of Gastroenterology and Hepatology, 2020, 35(7): 1215-22. DOI: 10.1111/jgh.14925.
[14] HAQUE L Y K, LIM J K. Budd-chiari syndrome: An uncommon cause of chronic liver disease that cannot be missed[J]. Clinics in Liver Disease, 2020, 24(3): 453-81. DOI: 10.1016/j.cld.2020.04.012.
[15] BONIFAZI F, BARBATO F, RAVAIOLI F, et al. Diagnosis and treatment of VOD/SOS after allogeneic hematopoietic stem cell transplantation[J]. Frontiers in Immunology, 2020, 11. DOI: 10.3389/fimmu.2020.00489.
[16] ZHUGE Y, LIU Y, XIE W, et al. Expert consensus on the clinical management of pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome[J]. Journal of GASTRoenterology and HEPatology, 2019, 34(4): 634-42. DOI: 10.1111/jgh.14612.
[17] UEDA K, MATSUI O, KADOYA M, et al. CTAP in budd-chiari syndrome: Evaluation of intrahepatic portal flow[J]. Abdominal Imaging, 1998, 23(3): 304-308. DOI: 10.1007/s002619900346.
[18] MILLER W J, FEDERLE M P, STRAUB W H, et al. Budd-Chiari syndrome: Imaging with pathologic correlation[J]. Abdominal Imaging, 1993, 18(4): 329-335. DOI: 10.1007/BF00201775.
[19] 唐栋, 王晓嫚, 丁建平, et al. 肝窦阻塞综合征的临床及影像学特点分析[J]. 医学影像学杂志, 2017, 27(6): 3. DOI:CNKI: SUN:XYXZ.0.2017-06-031. TANG D, WANG X M, DING J P, et al. Analyses of clinical and imaging features of hepatic sinusoidal obstruction syndrome[J]. Journal of Medical Imaging, 2017, 27(6): 3. DOI:CNKI: SUN:XYXZ.0.2017-06-031. (in Chinese).
[20] 郭严, 张世荣, 文良志, et al. 我国吡咯烷生物碱致肝窦阻塞综合征的临床特征分析[J]. 临床肝胆病杂志, 2018, 34(6): 1277-1281. DOI: 10.3969/j.issn.1001-5256.2018.06.029. GUO Y, ZHANG S R, WEN L Z, et al. Clinical features of sinusoidal obstruction syndrome induced by pyrrolidine alkaloids in China[J]. Journal of Clinical Hepatology, 2018, 34(6): 1277-1281. DOI: 10.3969/j.issn.1001-5256.2018.06.029. (in Chinese).
[21] 阳建军, 胡春洪, 何剑. 超声与CT诊断肝小静脉闭塞病的对比研究[J]. 医学影像学杂志, 2010, 20(9): 5. DOI: 10.3969/j.issn.1006-9011.2010.09.045. YANG J J, HU C H, HE J. The comparative study of ultrasond and CT in diagnosis of hepatic veno-occlusive disease[J]. Journal of Clinical Hepatology, 2010, 20(9): 5. DOI: 10.3969/j.issn.1006-9011.2010.09.045.
[22] 李红伟, 刘金朝, 黄勇华, et al. CT及DSA在肝小静脉闭塞症鉴别诊断中的应用[J]. 医学影像学杂志, 2017, 27(10): 4. DOI: CNKI:SUN:XYXZ.0.2017-10-028. LI H W, LIU J C, HUUANG Y H, et al. Application and research of CT and DSA in the differential diagnosis of hepatic venular occlusive disease[J]. Journal of Clinical Hepatology, 2017, 27(10): 4. DOI: CNKI:SUN:XYXZ.0.2017-10-028.
[23] 裴贻刚, 胡道予, 沈亚琪, 等. 多层螺旋CT与核磁共振成像对肝小静脉闭塞病的诊断价值[J]. 中华肝脏病杂志, 2010(2): 3. DOI: 10.3760/cma.j.issn.1007-3418.2010.02.018. PEI Y G, HU D Y, SHEN Y Q, et al. Multislice CT and magnetic resonance imaging diagnostic value of hepatic veno-occlusive disease[J]. Chinese Journal of Hepatology, 2010(2): 3. DOI: 10.3760/cma.j.issn.1007-3418.2010.02.018.
[24] DAI F, QIAO W, KANG Z, et al. Clinical features and CT imaging analysis of hepatic sinuscase-syndrome and budd-chiari syndrome[J]. International Journal of General Medicine, 2022, 15: 2389-2396. DOI: 10.2147/IJGM.S348176.
[25] 中国医师协会腔内血管学专业委员会腔静脉阻塞专家委员会. 布-加综合征亚型分型的专家共识[J]. 介入放射学杂志, 2017. DOI: CNKI:SUN:JRFS.0.2017-03-001. Expert Committee on Vena Cava Obstruction, Specialized Committee of Endovascology, Chinese Medical Doctor Association. Expert consensus on the classification of subtypes in Budd-Chiari syndrome[J]. Journal of Interventional Radiology 2017. DOI:CNKI:SUN:JRFS.0.2017-03-001. (in Chinese).
[26] MOHTY M, MALARD F, ABECASSIS M, et al. Revised diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in adult patients: a new classification from the European Society for Blood and Marrow Transplantation[J]. Bone marrow transplantation, 2016, (51-7).
[27] LIU S Y, LI T X, XIAO P, et al. Accuracy of computed tomographic angiography in the diagnosis of patients with inferior vena cava partial obstruction in Budd–Chiari syndrome[J]. Journal of Gastroenterology and Hepatology, 2016. DOI: 10.1111/jgh.13420.
[28] ZHUGE Y, LIU Y, XIE W, et al. Expert consensus on the clinical management of pyrrolizidine alkaloid‐induced hepatic sinusoidal obstruction syndrome[J]. Journal of Gastroenterology and Hepatology, 2019. DOI: 10.1111/jgh.14612.
[29] WANG X, ZHANG W, ZHANG M, et al. Development of a drum tower severity scoring (DTSS) system for pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome[J]. Hepatology International, 2022, 16(3): 669-679. DOI: 10.1007/s12072-021-10293-5.
[30] 中国研究型医院学会布-加综合征及肝脏血管病专业委员会. 中国巴德-吉亚利综合征多学科协作诊治专家共识(2021版)[J]. 中华外科杂志, 2022, 60(4): 8. DOI: 10.3760/cma.j.cn112139-20211224-00619. Budd-Chiari Syndrome and Hepatic Vascular Diseases Professional Committee of Chinese Research. Hospital Association Chinese multidisciplinary collaborative expert consensus for the diagnosis and treatment of Budd-Chiari syndrome (2021 version)[J]. Chinese Journal of Surgery, 2022, 60(4): 8. DOI: 10.3760/cma.j.cn112139-20211224-00619. (in Chinese).
[31] LI Z, WANG L, YI F, et al. Rapid development of gingival bleeding after rivaroxaban in a patient with Budd-Chiari syndrome[J]. Liver International, 2021, 41(9). DOI: 10.1111/liv.15021.



计量
- 文章访问数: 0
- HTML全文浏览量: 1
- PDF下载量: 0


